
Author: Andrews Dean, CPHIMS, CPHI, CHDA, CPPM, CPC, MACRA and MIPS Consultant
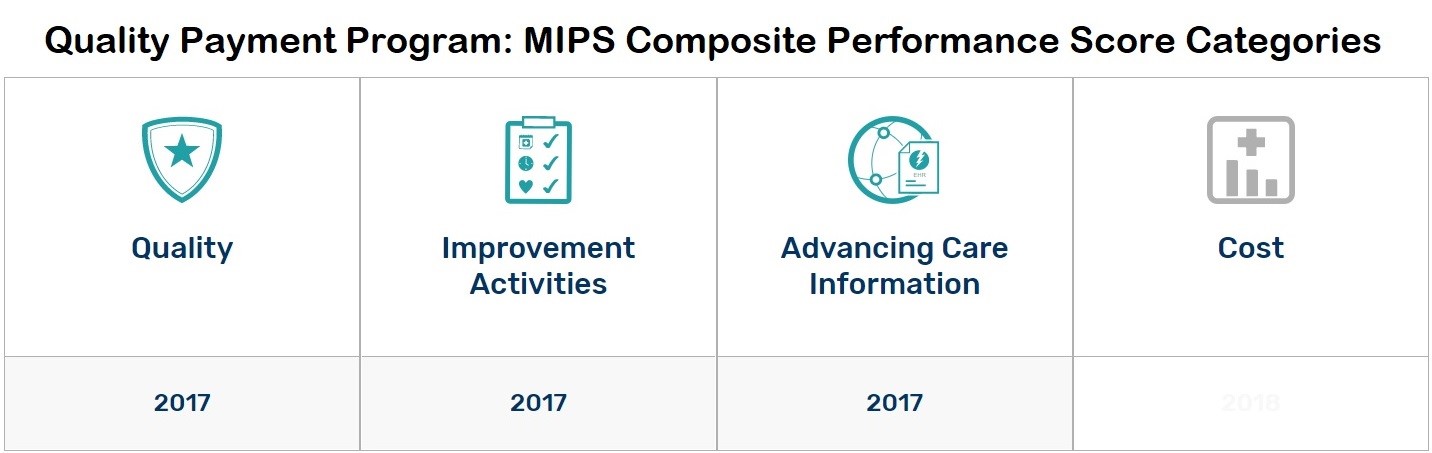
With Alternative Payment Model reporting tracks still undergoing growing pains, many physicians are expected to participate in the Merit-based Incentive Payment System for the MIPS integrates three outpatient payment programs—the Physician Quality Reporting System, Meaningful Use, and the Value-based Payment Modifier—with an assessment of Improvement Activities to establish an annual Composite Performance Score reflective of a clinician’s standing relative to peers. That score determines Medicare incentive or penalty payments for up to a 4 (+ or -) percent adjustment in 2019 and up to a 9 (+ or -) percent adjustment by 2022.
To meet reporting requirements under the program—and shed better light on opportunities for clinical performance improvement—providers are relying on Electronic Health Record technology and registries to capture and trend the necessary data. Reconfiguring existing EHR technology and clinical workflows to align with new QPP clinical quality measures while continuing to juggle day-to-day patient care has proven to be difficult for most practices. A study published by Health Affairs in 2016 found that the average practice spends 785 hours and $40,000 per physician per year reviewing and reporting quality data.
Awareness of the rising regulatory burden on providers prompted the Centers for Medicare and Medicaid Services to introduce “pick your pace” flexibilities in the program’s 2017 final rule. Now, updates proposed for the 2018 QPP reporting year, anticipated to be finalized late in 2018, seek to continue that trend.
2018 QPP Proposed Rule Updates
Recommended updates to the 2018 QPP reporting period seek to further simplify program participation for clinicians through additional flexibilities, new opportunities for bonus points, and reduced reporting burdens on small practices and rural providers.
Proposed MIPS reporting track updates include:
- Revised eligibility requirements – MIPS exemption thresholds move to <200 patients and <$90,000 in Medicare Part B volume.
- 2014 Certified EHR Technology allowances –Certified EHR use is still required but 2014 CEHRT is now permitted with bonus points available to those using 2015 CEHRT.
- Additional help for smaller practices – Practices with 15 or fewer eligible clinicians can apply for hardship exemptions in the Advancing Care Information category (formerly Meaningful Use) and can get up to five bonus points if the eligible clinician or group submits data on at least one performance category in the applicable performance period.
- Extended data submission flexibilities – “Pick your pace” reporting options carry into 2018 and clinicians may use multiple submission mechanisms within any one MIPS reporting category.
- Facility-based scoring options – Facility-based clinicians who have at least 75% of their covered professional services supplied in the inpatient hospital setting or emergency department can report through the facility they do most of their work at instead of the practice.
- Improvement bonus point opportunities – Clinicians are rewarded if they demonstrate quality category improvement from 2017 to 2018.
- Cost variables postponement – Cost category scores are pushed out another year, redistributing 2018 reporting period weighting to the quality category.
- New virtual group options – Solo practitioners and group practices with 10 or fewer eligible clinicians can report as virtual groups to share and reduce reporting burdens.
What does not change with the proposed rule are the measure requirements for MIPS quality and ACI categories. CMS did, however, propose to modify and add several measures to each category in efforts to include as many specialty measure options as possible.
With strong bipartisan support, MACRA is decidedly here to stay and commercial payers are expected to follow in the footsteps of CMS as they establish their own quality-based reimbursement frameworks. CMS has partnered with America’s Health Insurance Plans to create a Core Quality Measures Collaborative designed to cultivate consistency in measures and avoid reporting sprawl for providers.
Easier paths to penalty avoidance in 2017 and the additional leniencies slated for 2018 make this an ideal time for clinicians to finetune their QPP reporting processes. Providers who approach quality reporting as a long-term strategy as opposed to a side-project will undoubtedly find more success as the industry continues its march towards value-based care in the years to come.
Does your organization have the resources it needs to successfully navigate MIPS? Learn how Pivot Point can help with your value-based strategy.